
PROMPT Initiative Toolbox

The PROMPT toolbox is a one-stop shop for all of your PROMPT resources! Check back often for updates!
-
FPQC PROMPT Key Resources
- PROMPT Toolkit Document
- PROMPT Key Driver Diagram
- PROMPT Quick Start Guide
- 30-60-90 Day Plan
- 30-60-90 Day Plan Example
FPQC PROMPT Data Resources
-
Newest resources since January 2026
Driver 1: Readiness
- FPQC PROMPT Timely Treatment Flyer: This flyer promotes prompt treatment of severe hypertension in pregnancy and postpartum. The flyer provides the definition of persistent severe hypertension and examples of common clinical scenarios. The back page contains ACOG & SMFM resources and rationale for timely treatment within 60 minutes.
Driver 2: Recognition
Blood Pressure Cuff Patient Education Tools
-
1a: Develop standard protocols/processes for identification, management, and treatment of severe hypertension
Evidence/Rationale
- ACOG Practice Bulletin #222 Gestational Hypertension and Preeclampsia: ACOG recommends treatment for persistent, severe hypertension within 30-60 minutes.
- ACOG CO #667 Hospital-Based Triage of Obstetric Patients: ACOG recommends collaborating with other departments to create guidelines for triage of pregnant women in all hospital settings and standardized triage protocols.
- ACOG Practice Bulletin #203 Chronic Hypertension in Pregnancy: When antihypertensive therapy is used during pregnancy, an important consideration is the context of therapy, which is either 1) chronic treatment to lower blood pressure to maintenance levels, sometimes slowly during 24–48 hours often in the outpatient setting, or 2) acute lowering of critical hypertension in the hospital setting.
- Implementing Obstetric Early Warning Systems (Friedman et al. 2018)
Preeclampsia Tools
Eclampsia Tools
Algorithm and Policy Examples
- ACOG Hypertensive Emergency Checklist
- CMQCC Acute Treatment Algorithm
- AdventHealth Severe Hypertension in Pregnancy Treatment Algorithm
- AdventHealth Postpartum Blood Pressure Management from Delivery to Discharge
- Winnie Palmer Policy: Management of hypertensive disorders in pregnancy and postpartum
Nurse-Driven Protocols
ED and EMS Resources
- ACOG ED Postpartum Preeclampsia Checklist
- ACOG Identifying and Managing Obstetric Emergencies in Nonobstetric Settings
- ED Algorithm: Acute Hypertension in Pregnancy and Postpartum Algorithm
- ED Algorithm: Eclampsia
- EMS Information Sheet
- EMS Guideline: Elevated Blood Pressure in Pregnancy and Postpartum
- EMS Guideline: Eclampsia
- Florida EMS Protocol – Florida has begun roll out of an EMS Maternal Hypertension Protocol. If you are interested in working with your local EMS agency, ACOG EMS resources can be found above. Refer to FPQC’s Postpartum ER Resources page for additional ED resources.
1b: Ensure rapid access to severe hypertension medication
Timely Treatment
- ACOG Practice Bulletin #222 Gestational Hypertension and Preeclampsia: ACOG recommends urgent blood pressure control with antihypertensive medications such as labetalol, hydralazine and immediate release nifedipine.
- SMFM Special Statement: A quality metric for evaluating timely treatment of severe hypertension
- Identification of factors associated with delayed treatment of obstetric hypertensive emergencies (Kantorowska et al. 2020)
- Immediate release oral nifedipine for severe hypertension in pregnancy—Time for re-prioritization as a management option (Sarker et al. 2025)
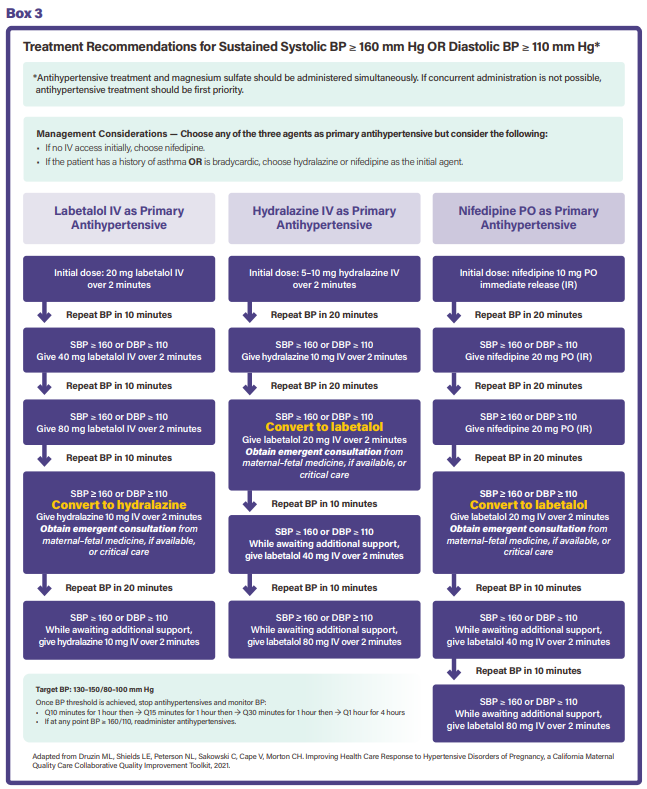
- ACOG Acute Hypertension in Pregnancy and Postpartum Algorithm Box 3 Treatment Recommendations
- TGH Postpartum Hypertension Algorithm
- Sarasota Memorial Tear Off Pads for Severe Hypertensive Emergency
- FPQC PROMPT Timely Treatment Flyer: This flyer promotes prompt treatment of severe hypertension in pregnancy and postpartum. The flyer provides the definition of persistent severe hypertension and examples of common clinical scenarios. The back page contains ACOG & SMFM resources and rationale for timely treatment within 60 minutes.
Medication Algorithms
Order Sets
- Semiautonomous Treatment Algorithm for the Management of Severe Hypertension in Pregnancy (Martin et al. 2021)
- EPIC Hypertension Order Set: Pregnant to 12 Weeks
- Winnie Palmer EPIC Order Sets
- BayCare Cerner Standing Orders
Medication Kit and Emergency Cart Examples
- FPQC Sample Acute-Onset, Severe Hypertension and Eclampsia Medication Kit: Sample Emergency Access Medication Kit for OB Patients with Severe Hypertension. Includes antihypertensives and seizure prophylaxis.
- CMQCC Sample Acute-Onset, Severe Hypertension and Eclampsia Medication Kit
- BUMED Obstetric Hemorrhage Cart Example: Standardized OB Emergency for Military Hospitals
- AdventHealth Tampa OB Emergency Cart
1c: Integrate a patient advisor on your QI team
FPQC Patient & Family Advisory Council Tools
- FPQC Involving Patients in QI One Pager
- FPQC Patient Family Advisory Council Implementation Checklist
- FPQC Patient Engagement YouTube Playlist
- TGH Patient/Family Advisor Brochure
Patient Engagement Implementation Guides
- Family Engagement at the Systems Level: A Framework for Action Family-centered care that involves patients at the individual and system-wide levels as allies in their care has been associated with improved quality and safety, cost savings, improved health outcomes, increased patient and provider satisfaction, and more effective policies.
- Alberta Health Guide to Patient Engagement
- Institute for Patient- and Family-Centered Care (IPFCC)
- AHRQ Guide to Patient and Family Engagement in Hospital Quality and Safety
- Working with Patient and Families as Advisors Implementation Handbook
- MoMMA’s Voices AIM Webinars: This webinar series builds on the MoMMA’s Voices Lived Experience Integration into QI Work Community of Learning and includes Navigating Risk Management with CANDOR, Working with Patients on QI Projects, and Holding Safe Spaces.
-
2a: Assess and document if patient presenting is pregnant or has been within the past year in all care settings
Evidence/Rationale
- The Florida Maternal Mortality Review Committee findings have noted an increase in maternal morbidity and mortality through 12 months postpartum secondary to HTN and its complications, which predominantly occur postpartum. This webpage provides a link to the 2-page report on severe hypertension outcomes.
- AWHONN and ENA joint statement on care of OB patient in ED: This position statement from AWHONN & ENA provides standards on caring for the OB patient outside of OB unit.
- ACOG/AHA statement on opportunities to reduce maternal risk postpartum: This joint statement provides guidance for hospitals to improve maternal outcomes.
- ACOG Identifying and Managing Obstetric Emergencies in Nonobstetric Settings: ACOG recommends screening for pregnancy in the last year in all non-obstetric settings. This ACOG resource also contains ED algorithms for care of OB patients in non-obstetric settings
FPQC Tools
- FPQC ED Signage: Information with visuals and QR codes for the most complications/diagnosis for postpartum period that links to guidelines for care.
- FPQC Wallet Card: Wallet card for patient information on date of giving birth, date of Post-Birth Health Check, provider contact, complications, and medications. Can be used as part of discharge education. Spanish and Haitian Creole versions are also available.
- PACC ED Triage EMR Example: An example of how the "have you been pregnant in the past year?" screening question has been incorporated into an EMR.
2b: Ensure accurate blood pressure measurement and assessment
Evidence/Rationale
- Hypertension in Pregnancy: Diagnosis, Blood Pressure Goals, and Pharmacotherapy: A Scientific Statement from the American Heart Association: The American Heart Association states: “Accurate blood pressure measurement is crucial for classifying hypertension and initiating treatment, regardless of pregnancy status.”
Definition of Persistent Severe Hypertension
- SMFM Special Statement: A quality metric for evaluating timely treatment of severe hypertension: Includes examples of persistent severe HTN
- PROMPT Data Webinar #1: Includes examples of persistent severe HTN and reviews SMFM Quality Metric.
BP Assessment Resources
- FPQC BP Assessment (PowerPoint Slides)
- FPQC BP Clinician Competency
- Clinician Infographics: BP Key elements
- AWHONN: Back to basics for clinicians on how to take an accurate blood pressure.
- Million Hearts: Compendium on hypertension in pregnancy. Infographic on page 11 explaining how to take an accurate BP.
2c: Provide verbal and written HTN education to patients and support persons
Evidence/Rationale
- ACOG CO #736 - Optimizing Postpartum Care: ACOG recommends patients and support persons receive education on warning signs for hypertensive disorders.
- ACOG CO #676 - Health Literacy to Promote Quality of Care: Learning preferences and levels of health literacy vary among patients. Materials accessible to all patients are essential to communicate with a diverse population (health literacy, multiple languages, appropriate reading level, infographic style).
Post-Birth Warning Signs Patient Education Tools
- AWHONN Post-Birth Warning Signs (PBWS) Digital Download: The AWHONN PBWS is an evidence-based tool that educates patients and families on warning signs and is available in over 23 languages. This digital download makes it easy for new parents to download and keep on their device for 1 year postpartum.
- AIM Urgent Maternal Warning Signs: This infographic can be used as a poster or handout for pregnant and PP patients with pictures of early warning signs
- CDC Hear HER: Free and comprehensive components for clinical teams to utilize (includes videos, patient stories)
- Patient Handout-Signs and Symptoms of Preeclampsia including Postpartum Preeclampsia: This webpage from The Preeclampsia Foundation educates patients on signs and symptoms of postpartum preeclampsia.
- Patient Handout: ACC Heart Health After Pregnancy: This one-page infographic educates PP patients on heart health with signs and symptoms to report.
Blood Pressure Cuff Patient Education Tools
- FPQC Wrist Cuff Patient Education. Spanish version.
- FPQC Arm Cuff Patient Education. Spanish version.
- Preeclampsia Foundation Video Link to Self-Measured Blood Pressure: This video demonstrates for patients how to take their own BP. Some hospitals load this on their hospital learning platform for ease of patient use.
Discharge Resources
- FPQC Wallet Card: Wallet card for patient information on date of giving birth, date of Post-Birth Health Check, provider contact, complications, and medications. Can be used as part of discharge education. Spanish and Haitian Creole versions are also available.
- 4th Trimester Resources: A list of postpartum resources, handouts, and videos. The 4th Trimester site is designed to provide the latest medical evidence and offer real, honest stories to inform postpartum planning. The information on the website has been reviewed by physicians, midwives, and nurses. However, we encourage women to always contact their health care provider with questions or concerns.
Tools for Clinical Teams
- AWHONN PBWS Online Course: The POST-BIRTH Warning Signs online course and program resources educate nurses and clinicians about postpartum maternal morbidity and mortality crises in the United States, and provides a respectful, evidence-based approach to postpartum pre- and post-discharge education for all patients, regardless of risk factors.
- Free Contact Hour AIM Severe Hypertension bundle: This free contact hour for both physicians and nurses is an online module which reviews the AIM Severe HTN bundle components.
- IHI Teach-Back Method: The Always Use Teach Back! tools can be used to confirm patient understanding of care instructions by asking patients to repeat the instructions using their own words. An extensive suite of tools is available for download from IHI.org.
- Health Literacy Module: This free course, presented in joint sponsorship with the Florida Perinatal Quality Collaborative and Baptist Health will equip perinatal care clinicians with key health literacy principles to apply to postpartum care. This will create a meaningful difference in patients’ postpartum health literacy, which will better prepare them for postpartum transitions; help them understand the importance of identifying early warning signs and post-birth health checks; facilitate follow-up and continuing care; and prioritize health literacy within healthcare organizations.
2d: Provide interdisciplinary clinician team training for early recognition and treatment of OB hypertensive emergencies (ED, OB, Cardiology, ICU)
Evidence/Rationale
- Joint Commission HR 11.03.01 EP 2 and 4: Applicable staff are trained annually on the protocols and provisions implemented for emergency services readiness and the hospital is able to demonstrate staff knowledge on the topics implemented.
Drills and Simulation Tools
- FPQC Sample Simulation
- Case: Woman Presents to ED with Headache and Hypertenstion (medscape.com): The CDC and Medscape have recently published a case challenge on postpartum preeclampsia. Authored by several experts across the country, including Dr. Carolyn Holland.
- CMQCC Simulation Scenarios
- AIM Obstetric In-Situ Drill Program Manual: This compendium published in 2022 is an additional resource for hospitals to utilize for developing in situ OB simulation drills.
- AWHONN Obstetric Patient Safety (OPS): Obstetric Emergencies Workshop 3rd Edition Flyer
- AWHONN Team Debriefing Form
-
3a: Implement standardized protocol for treatment of severe hypertension
Evidence/Rationale
- Joint Commission LD 13.01.01 EP 20-22: The hospital has adequate provisions and protocols consistent with nationally recognized and evidence-based guidelines to meet the emergency needs of patients.
- ACOG Practice Bulletin #222 Gestational Hypertension and Preeclampsia: ACOG recommends treatment for persistent, severe hypertension within 30-60 minutes.
- SMFM Hypertension in Pregnancy Change Package: SMFM recommends quality improvement and implementation of evidence-based tools to improve maternal morbidity and mortality.
Implementation Tools
- A refined compilation of implementation strategies: results from the Expert Recommendations for Implementing Change (ERIC) project (Powell et al. 2015)
- CMQCC Acute Treatment Algorithm with FPQC Implementation Tips
- CMQCC Stop Sign for ED (available in English and Spanish)
Workflows and Protocols
EHR Tools and Examples
- Cerner Standing Orders (Baycare)
- EPIC Hypertension Order Set: Pregnant to 12 Weeks
- Hypertension Workflow Example (Tampa General Hospital)
- Epic Guidelines: Patient Briefing & Discharge Paperwork (Lee Health)
- Cerner OB Post Events (Mease Countryside Hospital)
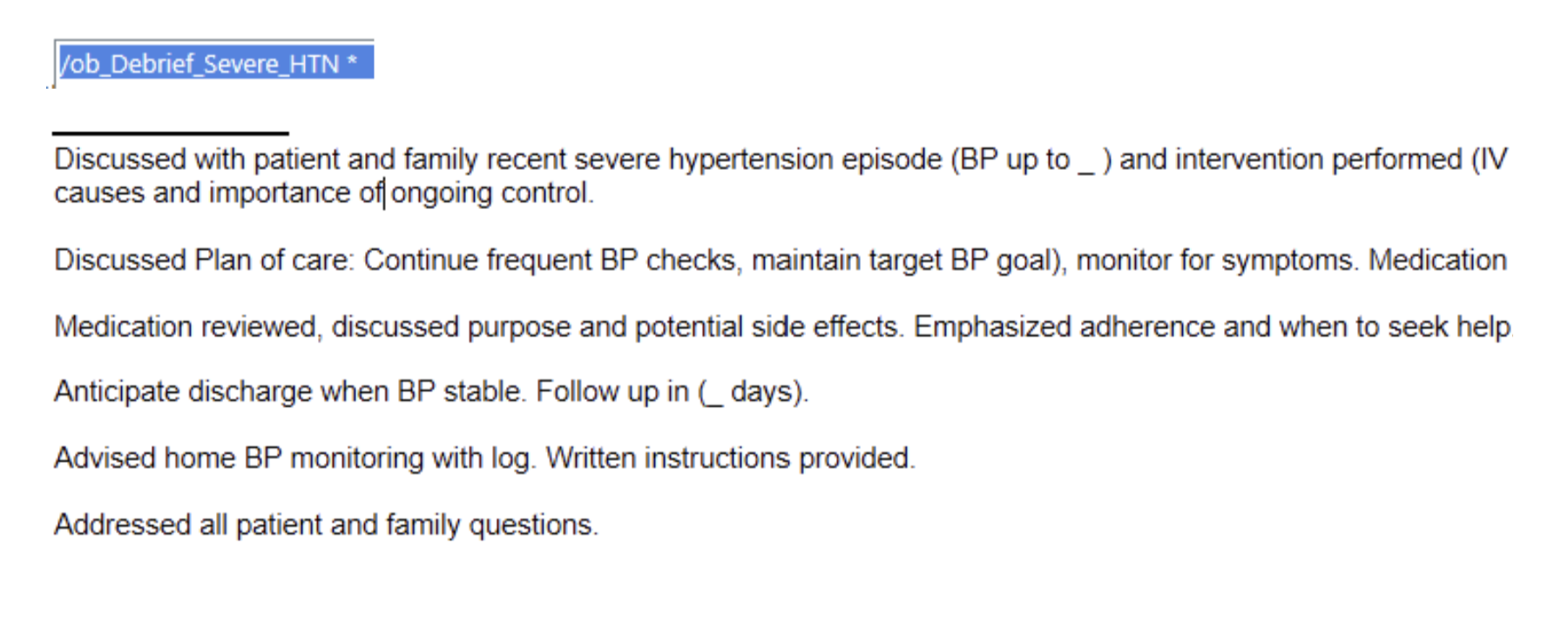
- Cerner Patient Brief Dot Phrase (Lakeland Regional Health)
Clinical Team Debrief Tools
3b: Provide trauma-informed support for patients
Evidence/Rationale
- ACOG CO #825- Caring for patients who have experienced trauma: ACOG recommends that the entire clinical team implements a trauma-informed approach in a physical and psychologically safe context when interacting with patients. This includes recognition of prevalence of trauma and effect on patients and providers, building a trauma-informed workforce, and universal screening for a history of and current trauma with attention to avoiding stigmatization and prioritizing resilience. Providers and hospital systems should also recognize the stress on providers caring for patients in traumatic events. Hospital systems may develop peer-to-peer counseling and debriefs to initiate the process of healing from events, identifying when additional resources are needed and preventing burnout.
Trauma Support for Patients
- Birth Trauma Resources (Preeclampsia Foundation)
- What to Expect in the Hospital (FPQC)
Trauma Support for Clinical Teams
- Second Victim Syndrome (Sachs & Wheaton, 2023)
- Trauma Care for Clinical Teams (TGH)
- Code Lavender guidelines (Stryker): This solution-focused toolkit outlines the importance of Code Lavender programs and how they can be implemented to support the physical, emotional and spiritual wellbeing of patients, families and care team members.
- Code Lavender: A Tool for Support Staff (Cleveland Clinic): Patients, family members, volunteers, and healthcare staff can call a Code Lavender when a stressful event or series of stressful events occurs in the hospital.
- Am I Providing Trauma-Informed Care? (FPQC): One-pager with actionable strategies for clinical teams.
Patient Briefs
- Patient Brief vs Clinical Team Debrief Slides
- PROMPT Patient Brief Sample Script
- PROMPT Patient Brief Guidelines and Checklist for RN and Provider
- Epic Guidelines: Patient Briefing & Discharge Paperwork (Lee Health)
- Cerner OB Post Events (Mease Countryside Hospital)
- Cerner Patient Brief Dot Phrase (Lakeland Regional Health)
3c: Schedule postpartum encounter 3-7 days after discharge
Evidence/Rationale
- ACOG CO #736 - Optimizing Postpartum Care: ACOG recommends that patients with hypertensive disorders of pregnancy have a BP check in 3-7 days postpartum and receive education on warning signs for hypertensive disorders.
- Pregnancy-Associated Stroke and Outcomes Related to Timing and Hypertensive Disorders (Bitar et al. 2023): Patients who suffer from hypertension are at an increased risk for stroke. It is important that patients are educated on these risks and symptoms, and they may require additional monitoring throughout the postpartum period and beyond.
FPQC Discharge Tools
- Adapted from PACC:
- Adopted from PACC:
- Maternal Discharge Assessment
- Postpartum Discharge Assessment
- Scheduling Postpartum Visit Sample (TGH)
- FPQC My Post-Birth Wallet Card: Wallet card for patient information on date of giving birth, date of Post-Birth Health Check, provider contact, complications, and medications. Can be used as part of discharge education. Spanish version. Haitian Creole version.
Post-Birth Health Check Resources
- Adopted from PACC:
- Post-Birth Heath Check Billing/Coding: To share with OB provider offices which details strategies necessary to receive additional reimbursement for the early postpartum visit.
- Updated Post-Birth Health Check: Follow the B's!: Checklist for providers to utilize during the postpartum visit and to display in clinics. There are also patient-facing versions in Spanish, and Haitian Creole.
Additional Resources
-
Respectful maternity care (RMC) is a universal component of every PROMPT driver and activity. Here are some RMC resources for your hospital teams:
Strategies and Guidelines
- ACOG Committee Opinion #587: Effective Patient–Physician Communication: Physicians’ ability to effectively and compassionately communicate information is key to a successful patient–physician relationship. The use of patient-centered interviewing, caring communication skills, and shared decision making improves patient–physician communication. Involving advanced practice nurses or physician assistants may improve the patient’s experience and understanding of her visit.
- Respectful Maternity Care Implementation Toolkit (RMC-IT [AWHONN]): The Respectful Maternity Care Implementation Toolkit (free for AWHONN members and available for a small fee for non-members) provides the tools and resources needed to implement the 10-Step “C.A.R.E. P.A.A.T.T.H.” within organizations. Make the commitment today to provide Respectful Maternity Care to every patient, every interaction, every time.
- New York City Standards for Respectful Care at Birth: This brochure is useful for both patients and providers and discusses shared decision-making and respect for human rights during pregnancy, labor, and childbirth.
- The International Childbirth Initiative (ICI): The 12 Steps (summary version) to Safe and Respectful MotherBaby-Family Maternity Care
Reference Articles and Reports
- Operationalizing respectful maternity care at the healthcare provider level: a systematic scoping review: Ensuring the right to respectful care for maternal and newborn health, a critical dimension of quality and acceptability, requires meeting standards for Respectful Maternity Care (RMC). Absence of mistreatment does not constitute RMC. Evidence generation to inform definitional standards for RMC is in an early stage. The aim of this systematic review is clear provider-level operationalization of key RMC principles, to facilitate their consistent implementation.
- Exploring Evidence for Disrespect and Abuse in Facility-Based Childbirth: Reports from a Landscape Analysis (USAID): This is an important review by Bowser and Hill of the evidence on the topic of disrespect and abuse in facility based childbirth. The primary purpose of the report is to review the evidence in published and gray literature with regard to the definition, scope, contributors, and impact of disrespect and abuse in childbirth, to review promising intervention approaches, and to identify gaps in the evidence.
- Respectful Maternity Care: The Universal Rights of Childbearing Women (White Ribbon Alliance): By design, this document focuses specifically on the interpersonal aspects of care received by women seeking maternity services. A woman’s relationship with maternity care providers and the maternity care system during pregnancy and childbirth is vitally important. Not only are these encounters the vehicle for essential and potentially lifesaving health services, women’s experiences with caregivers at this time have the impact to empower and comfort or to inflict lasting damage and emotional trauma, adding to or detracting from women’s confidence and self‐esteem. Either way, women’s memories of their childbearing experiences stay with them for a lifetime and are often shared with other women, contributing to a climate of confidence or doubt around childbearing.
Refer to the MFC Respectful Care Driver in the MFC Toolbox for additional resources.
{kind=link}
{kind=link}
{kind=link}