
USF Health utilizes the latest technology to perform these minimally invasive procedures with reduced risks for our patients. Surgical outcomes are improved at high-volume centers where dedicated expertise and experience reduce length of stay and reduce complications and maximize stone-free rates. We are in the 90th percentile based on stone surgery volumes in the country.
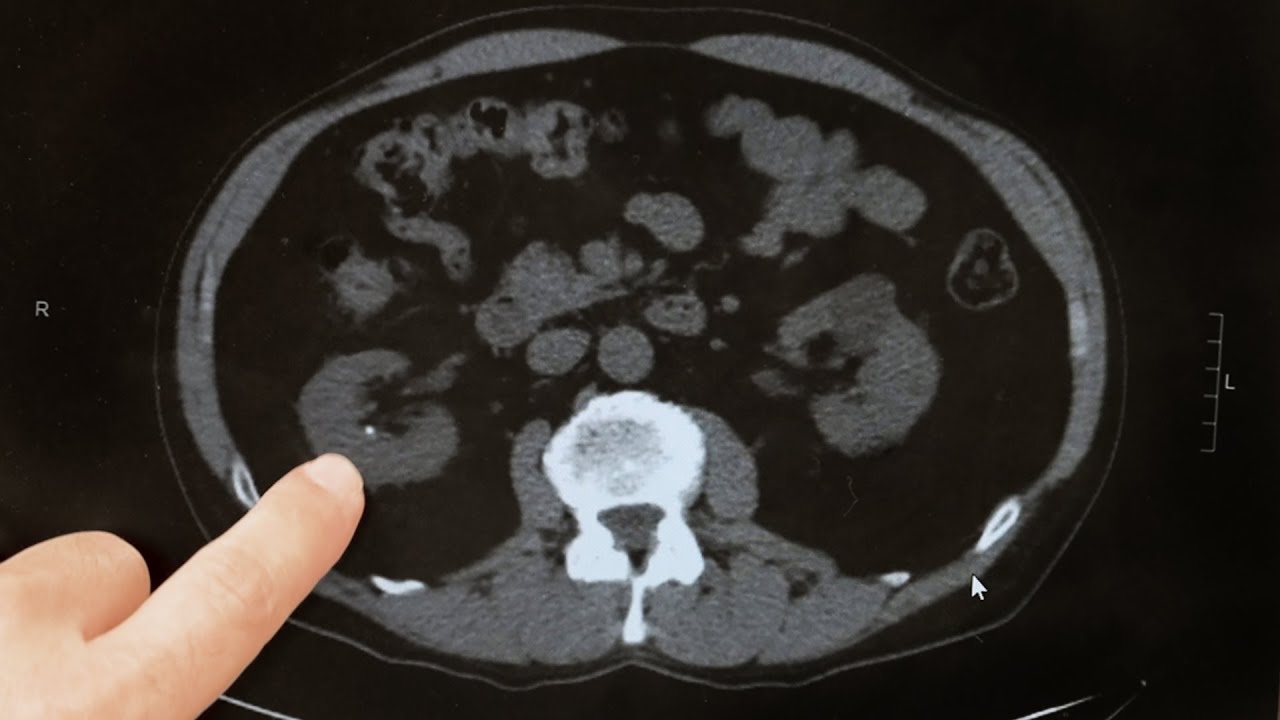
One out of every 10 Americans — and even more in the southeast — suffer from kidney stones. Though common, this unpredictable and painful condition has a high risk of returning, with more than half of patients experiencing stone recurrence within five years. Patients often require surgery, and have an increased risk of infections and loss of kidney function.
Providing comprehensive care through a team of experts to treat and prevent the recurrence of painful kidney stones. By uniting medical and health experts from a combination of specialties, stone recurrence can be prevented. Most urology practices do not have the resources to focus on prevention, and there is no kidney stone center in the Tampa Bay region. USF Health has the expertise to transform the care of Florida patients with the vision to make it a reality.
When a kidney stone causes uncontrolled pain, severe nausea or vomiting or is associated with a solitary kidney, poor kidney function or severe blockage of the kidney, the stone should be treated urgently. Obstructing stones associated with infection or fever can be life threatening and demand immediate decompression with either a nephrostomy tube or ureteral stent.
With small stones in the ureter, it may be appropriate give the stone a few weeks to pass on its own. Ureteral stones larger than 5 mm are less likely to pass spontaneously and should be considered for treatment. A trial of spontaneous passage is typically limited to 6 weeks or less to avoid kidney damage.
Small kidney stones (less than 5 mm) not causing any pain are often observed as there is a good chance these stones will pass spontaneously when they fall] into the ureter. However, there are a number of reasons to treat a kidney stone even if it is not causing pain. Some kidney stones may be infected, and in many cases, despite proper antibiotic treatment, the infection cannot be cleared from the stone. In such cases, the only way to eradicate the infection completely is to remove the stone. Staghorn stones are extremely large stones that grow to fill the inside of the kidney. There are serious health risks associated with these stones and left untreated they are associated with an increased risk of kidney failure. There are also additional situations in which even small stones should be treated. For example, the Federal Aviation Administration (FAA) will not allow a pilot to fly until all stones have been cleared from his or her kidney. A few other occupations also do not allow for the unplanned passage of a kidney stone. Likewise, frequent travelers, whether for business or otherwise, especially to places where medical care is not reliable, should consider treatment. Others may choose to remove their stones at a time when it is convenient for them in order to avoid the unpredictable future passage.
Shock wave lithotripsy (SWL) is a noninvasive procedure used to treat kidney stones that are too large to pass through the urinary tract. SWL treats kidney stones by sending focused ultrasonic energy or shock waves directly to the stone first located with fluoroscopy (a type of X-ray) or ultrasound (high frequency sound waves). The shock waves break a large stone into smaller stones that will pass through the urinary system. SWL allows persons with certain types of stones in the urinary system to avoid an invasive surgical procedure for stone removal.
The introduction of shock wave lithotripsy in the early 1980s revolutionized the treatment of patients with kidney stone disease. Patients who once required major surgery to remove their stones could be treated without an incision. SWL is the only non-invasive treatment for kidney stones, meaning no incision or internal manipulation is performed. Shock wave lithotripsy involves the administration of a series of shock waves to the targeted stone. The shock waves, which are generated by a machine called a lithotripter, are focused by x-ray onto the kidney stone. The shock waves travel into the body, through skin and tissue, reaching the stone where they break it into small fragments. For several weeks following treatment, those small fragments are passed out of the body in the urine.
In the decades since lithotripsy was first performed in the United States, we have learned a great deal about how different patients respond to this technology. It turns out that we can identify some patients who will be unlikely to experience a successful outcome following lithotripsy, whereas we may predict that other patients will be more likely to clear their stones. Although many of these parameters are beyond anyone's control, such as the stone size and location in the kidney, patient selection and physician experience can positively influence the outcome of the procedure.
Ureteroscopy is a procedure to address kidney and ureteral stones, and involves the passage of a small telescope, called a ureteroscope, through the urethra and bladder and up the ureter to the point where the stone is located. Ureteroscopy is typically performed under general anesthesia, and the procedure usually lasts from one to three hours. If the stone is small, it may be snared with a basket device and removed whole from the ureter. If the stone is large, or if the diameter of the ureter is narrow, the stone will need to be fragmented, which is usually accomplished with a laser. Once the stone is broken into tiny pieces, these pieces are removed.
The passage of the ureteroscope may result in swelling in the ureter. Therefore, it may be necessary to temporarily leave a small tube, called a ureteral stent, inside the ureter temporarily to ensure that the kidney drains urine well. If a stent is placed, follow up for stent removal is critical.
Ureteroscopy usually can be performed as an outpatient procedure, however; patients may require an overnight hospital stay if the procedure proves lengthy or difficult.
Ureteroscopy can treat stones located at any position in the ureter and kidney. Additionally, ureteroscopy allows the treatment of stones that cannot be seen on an x-ray. Certain patients who cannot be treated with ESWL or PERC, such as those who cannot safely stop taking blood thinners, women who are pregnant, and the morbidly obese, can be treated by ureteroscopy.
Ureteroscopy is not a particularly good treatment for:
PCNL is a technique used to remove certain stones in the kidney or upper ureter (the tube that drains urine from the kidney to the bladder) that are too large for other forms of stone treatment such as shock wave lithotripsy or ureteroscopy.
This procedure is accepted as the standard of care for patients with kidney stones that are large, very firm, or resistant to other forms of stone treatment. It has replaced open operations for kidney stones in the vast majority of patients. Typically, the length of the surgery is three to four hours. The surgery is performed by making a small 1 cm incision in the patient’s flank area. A tube is placed through the incision into the kidney under x-ray guidance. A small telescope is then passed through the tube in order to visualize the stone, break it up and remove it from the body. If necessary a laser or other device called a lithotripter may be used to break up the stone before it can be removed. This procedure has resulted in significantly less post-operative pain, a shorter hospital stay, and earlier return to work and daily activities when compared to open stone surgery.
This technique also has a higher success rate for clearing all stones in one setting than other techniques such as extracorporeal shock wave lithotripsy (ESWL), which often require several attempts. Although this procedure has proven to be very safe, as in any surgical procedure there are risks and potential complications. The safety and complication rates are similar when compared to the open surgery.
 Elias Doumit, MD
Elias Doumit, MD
 Hariharan Ganapathi, MD
Hariharan Ganapathi, MD
 Kevin Heinsimer, MD
Kevin Heinsimer, MD
 David Hernandez, MD
David Hernandez, MD
 Elizabeth Norby, PA-C
Elizabeth Norby, PA-C
 Karina Falcone, MS, RD, LD, DipACLM
Karina Falcone, MS, RD, LD, DipACLM
Registered Dietician